Uterine Anomalies – Types, Impact on Fertility & Treatment
The shape of the uterus has a direct impact on the reproductive function, as it is the place where the embryo grows during the 9 months of pregnancy. Uterine or Müllerian duct anomalies (MDAs) are caused by alterations in the development of the uterus, causing implantation failure and recurrent pregnancy loss. As a consequence, some women with uterine anomalies have no alternative but to use a gestational surrogate to have a baby.
Some of the most common uterine malformations include bicornuate uterus, uterus didelphys, and septate uterus, amongst others. The following is a guide to the different types of uterine abnormalities, their causes, and their impact on female fertility, as well as the potential treatment options to start a family.
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 3.4.
- 3.5.
- 3.6.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 6.
Congenital uterine anomalies
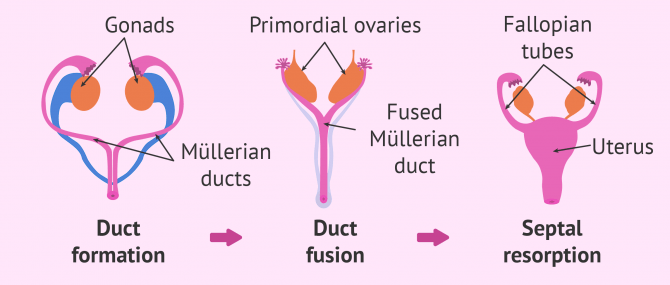
The uterus is formed from embryonic structures known as Müllerian ducts. During embryo development, the Müllerian ducts grow to form the main parts of the female reproductive system: uterus or womb, Fallopian tubes, cervix, and part of the vagina.
The differentiation of the female reproductive tract occurs in three stages:
- Formation of the Müllerian ducts
- Fusion of the ducts
- Resorption or elimination of the septum that divided them
In the case of male fetuses, the Müllerian ducts disappear due to the effect of the anti-Müllerian hormone. This is the reason why men don't have a womb and therefore can't get pregnant.

Any abnormality or alteration that occurs during embryo development may lead to developing a congenital uterine anomaly. As a result, the woman grows with an abnormally shaped uterus due to an incomplete Müllerian duct development.
Causes, symptoms & fertility
Abnormalities during Müllerian duct differentiation may be due to birth defects or prenatal environmental factors, including:
- Radiation exposure while pregnant
- Intrauterine infections
- Teratogenic substances, like diethylstilbestrol (DES)

Uterine abnormalities are present in about 5.5% of the current female population. Out of the women who undergo fertility treatment, this percent increases to 8%. And out of those who have suffered recurrent miscarriages or have been diagnosed with unexplained infertility, this figure soars to 24.5%.
In conclusion, and as one shall see, Müllerian duct malformations may compromise a woman's ability to get pregnant and carry a child until birth, being a major cause of recurrent miscarriage. Their impact on reproductive function depends on the type of anomaly and its grade of severity.
A large number of patients with anomalies of the uterus have no symptoms. As a consequence, they do not realize that they have an anomaly until they get a routine transvaginal ultrasound done or visit a fertility specialist due to trouble getting pregnant. The symptoms may vary based on the type of abnormality and its severity, though.
Types of uterine anomalies
The range of uterine shapes that can develop as a result of abnormal embryonic development can be classified into several types. The following are the most common ones:
Müllerian agenesis
By Müllerian agenesis or hypoplasia we refer to a congenital malformation characterized by a failure of the Müllerian duct to develop, which leads to a condition called Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome. These patients lack Fallopian tubes, cervix, and part of the vagina as well.
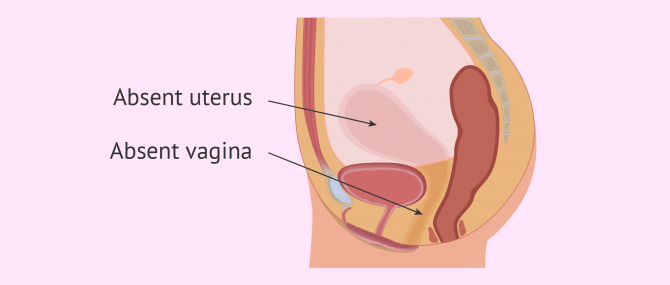
Luckily, these women have functional ovaries, which translates into ovulation and production of egg cells. However, they won't have normal menstrual periods (amenorrhea), as they lack the necessary organs for the menstrual cycle to happen monthly.
MRKH syndrome is diagnosed before age 20 in most cases, as soon as these women realize that they haven't had their first menstrual period. Painful intercourse (dyspareunia) or even the inability to have penetrative sex due to the partial absence of a vagina are two common symptoms of this condition too.
The particular causes of MRKH syndrome are still unknown. Some hypotheses, however, suggest that several genes and factors may be involved, like the absence of certain sex hormone receptors in the Müllerian ducts.
Women with Müllerian agenesis have no choice but to use a gestational carrier to have a biological child. Another option is uterine transplantation, but it is still an experimental technique. One should not forget that being born without a womb doesn't translate into not producing eggs.
Read more: What Is MRKH Syndrome? - Causes, Symptoms & Treatment.
Unicornuate uterus
In this case, one only of the paired Müllerian ducts develops. As a result, the uterus is smaller than normal, with a curved and elongated shape, and a unique Fallopian tube. Visually, the external uterine contour resembles a banana. It is diagnosed in 20 percent of the cases.
A unicornuate uterus can be classified into four subtypes:
- Without rudimentary uterine horn (35% of the cases)
- With communicating uterine horn containing a functional endometrium (10%)
- With non-communicating uterine horn containing a functional endometrium (22%): it can cause endometriosis and adenomyosis.
- With rudimentary horn that is non-functional (33%)

One should not forget that, even though these females have a single horn, they normally have two ovaries and in some cases two tubes.
Although it's not impossible, bearing a pregnancy with this type of anomaly is unlikely. In women who achieve an ongoing pregnancy, the risk of C-section, preterm delivery, and ectopic pregnancy increases dramatically. So, we can say that having a unicornuate uterus may affect female fertility to a large extent.
Uterus didelphys
Also known as uterus didelphis or double uterus, this abnormality counts for 5% of the cases of uterine malformations. It is diagnosed when both ducts develop but fail to fuse, resulting in two separate cervices.
We can distinguish two types of uterus didelphys:
- Uterus didelphys bicollis
- Each uterine cavity has an independent cervix and a vagina. It occurs in two-thirds of the cases.
- Uterus didelphys unicollis
- There are two uterine cavities that communicate between each other through the cervix, and there is only one vagina.
Broadly speaking, if there is no blockage in the vagina, this malformation is asymptomatic. However, it is associated with recurrent miscarriages and preterm births.

Although surgery can be used as a treatment option for uterus didelphis, it doesn't always lead to positive outcomes. There have been a number of studies with conflicting results on this matter.
In any case, females with this anomaly can achieve successful pregnancies depending on the size and reproductive function of both cavities. For example, a woman in England was able to give birth to triplets from two separate wombs.
Bicornuate uterus
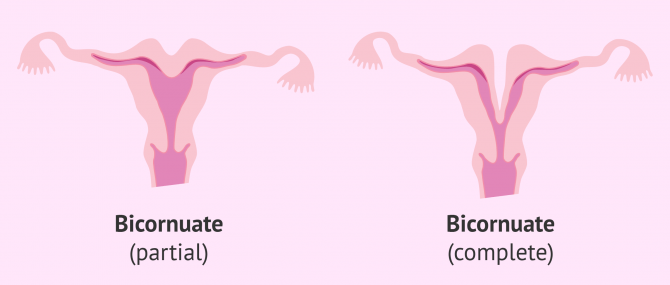
Bicornuate uterus commonly referred to as heart-shaped uterus, is caused by an incomplete lateral fusion of the Müllerian ducts. These women have two symmetric uteri, but the horns are underdeveloped and smaller than in cases of uterus didelphys.
Bicornuate uteri don't have the common pear shape of a normal uterus, but rather resemble a heart, hence the name. The horns are separated by a central septum, which reduces the space available for fetal development.
Depending on the extension of the dividing septum, we can differentiate between two subtypes:
- Complete bicornuate uterus
- It has a complete transverse vaginal septum that extends to the internal cervical orifice of the uterus (unicornuate bicollis) or the external cervical orifice of the uterus (bicornuate bicollis).
- Partial bicornuate uterus
- It just extends to the internal orifice of the uterus.
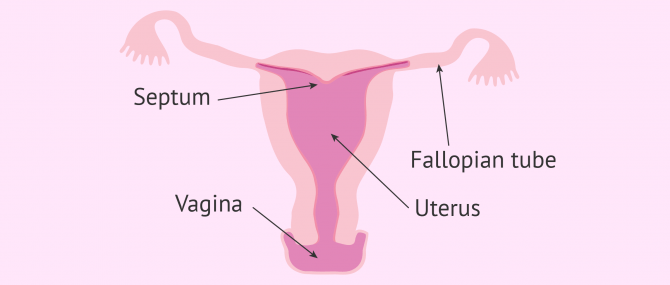
Septate uterus
Diagnosed in 55% of the patients that have an abnormality of the uterus. In this case, the septum that divided the Müllerian ducts doesn't disappear, resulting in a partitioned uterine cavity. The longitudinal septum may involve the endometrial canal but not the cervix (partial septate uterus), or extend to the internal or external cervical orifice of the uterus (complete septate uterus).

The difference with a bicornuate uterus is that in this case, the uterus is very much like a normal uterus, which is to say, shaped like an inverted pear.
This is the most common uterine abnormality and at the same time the one causing more cases of female infertility. In the most serious cases—those that cannot be treated with surgery—, a pregnancy could be considered dangerous due to the high risk of recurrent miscarriage.
Arcuate uterus
Some consider it a variation of the septate uterus, while others see it as just a mildly variant shape of the normal uterus. The main difference with the former is that the septum is less acute. This is precisely the reason why, in the mildest cases, the morphology of an arcuate uterus is similar to a normal uterus.
This uterine anomaly is rather common. It rarely causes infertility, although it may take longer for the woman to get pregnant (subfertility). If it leads to recurrent miscarriages, it can be treated with surgery.
How to get pregnant
Some of the uterine abnormalities explained above can affect the transportation of gametes (eggs and sperm), but not necessarily the processes of embryo implantation and subsequent development. In such cases, In Vitro Fertilization (IVF) would allow the woman to become pregnant.
When IVF is the treatment option of choice, the specialist will perform a mock embryo transfer cycle prior to the actual cycle. The goal is to determine if there exists a blockage in the uterus that should be treated surgically. Also, it allows the specialist to examine if there is enough space within the uterine cavity for embryo growth.
On the other hand, certain anomalies of the uterus require surgery. For instance, in the case of septate uterus, a surgical procedure to remove the septum is required. Nonetheless, the extension of the malformation should be evaluated in order to determine its impact on reproductive function and pregnancy. To this end, methods such as MRI (Magnetic Resonance Imaging) allow specialists to detect and classify the different types of anomalies.
Based on the grade of severity, your doctor should consider the risk-benefit ratio carefully before making any decision. A potential side effect associated with surgery to treat Müllerian duct anomalies is damage to the uterine walls, which would increase the risk of implantation failure.
The good news is that the latest surgical procedures, including hysteroscopy and laparoscopy, remove the need for the surgeon to open the abdomen, which reduces the number of risks involved to a large extent.
Finally, when neither IVF nor surgery leads to successful outcomes, using a gestational surrogate may be an option. In this case, the surrogate carries a fetus until birth that has been created using the eggs of the intended mother.
Surrogacy is the assisted reproduction treatment that generates the most deception and doubts. Therefore, it is essential to choose a clinic and an agency that transmits transparency and avoids deception.
FAQs from users
What types of uterine abnormalities have the worst prognosis?
The more common congenital uterine anomalies (CUA) include uterine didelphis, bicornuate, unicornuate, septate. CUA are not thought to impair conception or implantation with IVF but to have an increase in miscarriages, intrauterine growth retardation, preterm delivery, malpresentation, cesarean delivery, rupture of a rudimentary horn, cervical incompetence, pregnancy induced hypertension and placental attachment abnormalities. It is thought that CUA occur in about 8% of infertile women. There is no surgical treatment for CUA other than resecting a septum or excising a rudimentary horn.
Are uterine anomalies associated with kidney abnormalities?
Yes, they are. Müllerian anomalies are frequently associated with anomalies of the renal tract. For example, a woman with a bicornuate uterus may have a solitary kidney. Also, a missing kidney and other kidney problems may accompany a unicornuate uterus.
What is a septum in the uterus?
A septum is a piece of tissue that can divide all or part of he uterine cavity in two halves. It is often an upside-down, triangular shaped piece of tissue.
Can a woman have two wombs?
Yes. During fetal development, the uterus starts out as two small tubes (Müllerian ducts). If these tubes don't join completely to create one larger organ (i.e. the uterus), the result is a separate structure known as uterus didelphys or double uterus.
Suggested for you
Surrogacy can be chosen as a last resort when IVF doesn't work to get pregnant with a uterine anomaly. When a woman is unable to get pregnant or causes recurrent miscarriages, using a gestational carrier may be the only option to be a mother. Learn more: What Is IVF Surrogacy? – Process, Success Rates & Cost.
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!